
Introduction
Facelift surgery remains one of the most effective interventions for addressing age‑related facial soft‑tissue descent. Contemporary techniques, most notably the deep‑plane facelift and SMAS (superficial musculoaponeurotic system) plication, differ in the anatomical plane of dissection, the degree of soft‑tissue mobilization, and the balance between longevity of results and perioperative morbidity. Understanding these differences is essential for plastic surgeons and related clinicians who counsel patients about long‑term outcomes, safety, and realistic expectations. This review synthesizes current evidence and practical guidance relevant to the U.S. clinical environment, with attention to objective outcome metrics and patient selection.
1. Comparative Analysis of Deep‑Plane vs. SMAS Plication Techniques
The deep‑plane facelift repositions the malar fat pad and midface by releasing deep attachments and mobilizing tissue below the superficial musculoaponeurotic system. Proponents cite superior midface rejuvenation and tension redistribution on durable deep tissues, which can translate into longer‑lasting contour improvement. In contrast, SMAS plication involves folding or imbricating the superficial fascial layer (SMAS) with less extensive dissection, typically producing reliable lower‑face and neck tightening with reduced operative time and potentially lower immediate surgical morbidity.
Reported durability differences are consistent across multiple cohort studies and reviews: deep‑plane approaches often demonstrate longer maintenance of midface and malar contour, with many series reporting meaningful aesthetic benefit at 7–10+ years; SMAS plication commonly yields durable improvement for 5–8 years depending on patient factors and technical execution. These ranges are derived from aggregated cohort follow‑ups and systematic reviews; individual results vary with patient age, skin quality, lifestyle factors (e.g., smoking, sun exposure), and surgeon technique. For a comprehensive overview of technique descriptions and outcomes, see clinical summaries such as those available from the American Society of Plastic Surgeons (ASPS) and peer‑reviewed literature on PubMed (https://www.plasticsurgery.org, https://pubmed.ncbi.nlm.nih.gov).
Advantages and limitations can be summarized as follows:
- Deep‑plane facelift: Advantages—more robust midface elevation, improved malar projection, and potentially longer durability. Limitations—greater technical complexity, longer operative time, and potentially increased short‑term swelling and bruising.
- SMAS plication: Advantages—shorter operative time, less invasive dissection, and faster early recovery for many patients. Limitations—may provide less durable midface elevation and a greater need for revision in patients with advanced tissue laxity.
Clinical decision‑making should weigh anatomical goals (midface vs. lower face/neck), patient comorbidities, and tolerance for postoperative downtime. Comparative registries and single‑center series provide useful guidance but highlight the need for randomized or prospectively matched studies to limit selection bias.
2. Systematic Review of Complication Rates and Recovery Profiles
Safety and recovery are central to technique selection. Major complications after facelift surgery are uncommon but clinically significant when they occur. Published literature reports variable rates depending on study design and patient selection; typical complication considerations include hematoma, infection, sensory or motor nerve injury, skin necrosis (rare), and the need for revision surgery.
Typical complication ranges reported across contemporary series and reviews include:
| Complication | Reported Range (selected literature) |
|---|---|
| Hematoma | ~1–8% |
| Infection | <1%–2% |
| Facial nerve injury (temporary) | ~1–5% |
| Permanent motor nerve injury | <1% |
| Revision surgery | ~2–6% |
These ranges reflect pooled data and should be interpreted in context: hematoma risk correlates with perioperative blood pressure control, anticoagulant use, smoking, and extent of dissection; hematoma rates tend to be higher in more extensive dissections such as deep‑plane approaches in some series. Infection and permanent nerve injury are rare in experienced hands. Surgeons should review institution‑level data and published benchmarks (for example, national reports available through professional societies) when counseling patients.
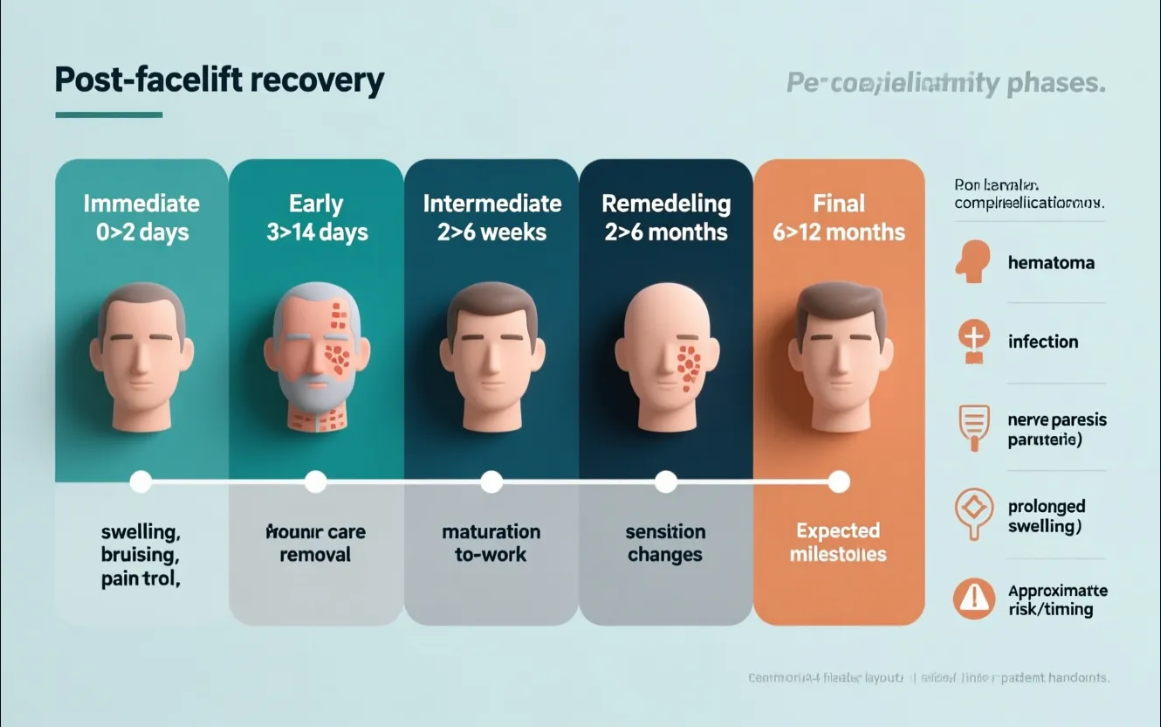
Recovery timelines vary by technique and individual patient factors. Broadly:
- SMAS plication and limited incision/mini‑facelift variants: many patients return to non‑strenuous activities and office work within 7–14 days, with residual swelling and contour maturation over weeks to months.
- Deep‑plane facelift: early recovery may involve greater initial swelling and ecchymosis, with an anticipated return to routine activities commonly between 2–3 weeks; contour refinement and final results typically mature over 3–6 months.
Pain is usually manageable with multimodal analgesia, and most patients report moderate discomfort in the first 48–72 hours with rapid decline thereafter. Early patient education about expectations for bruising, numbness, and temporary contour irregularities reduces postoperative anxiety and improves perceived recovery.
3. Objective Assessment of Aesthetic Outcomes
Objective outcome measurement is essential for comparing techniques and improving quality. Validated instruments such as the FACE‑Q patient‑reported outcome measures provide structured assessment of domains including satisfaction with facial appearance, psychosocial function, and quality of life after facial aesthetic procedures (see https://www.qportfolio.org/face-q/). Incorporating standardized patient‑reported outcome measures into routine practice allows clinicians to correlate procedural variables with patient satisfaction and to monitor long‑term benefit.
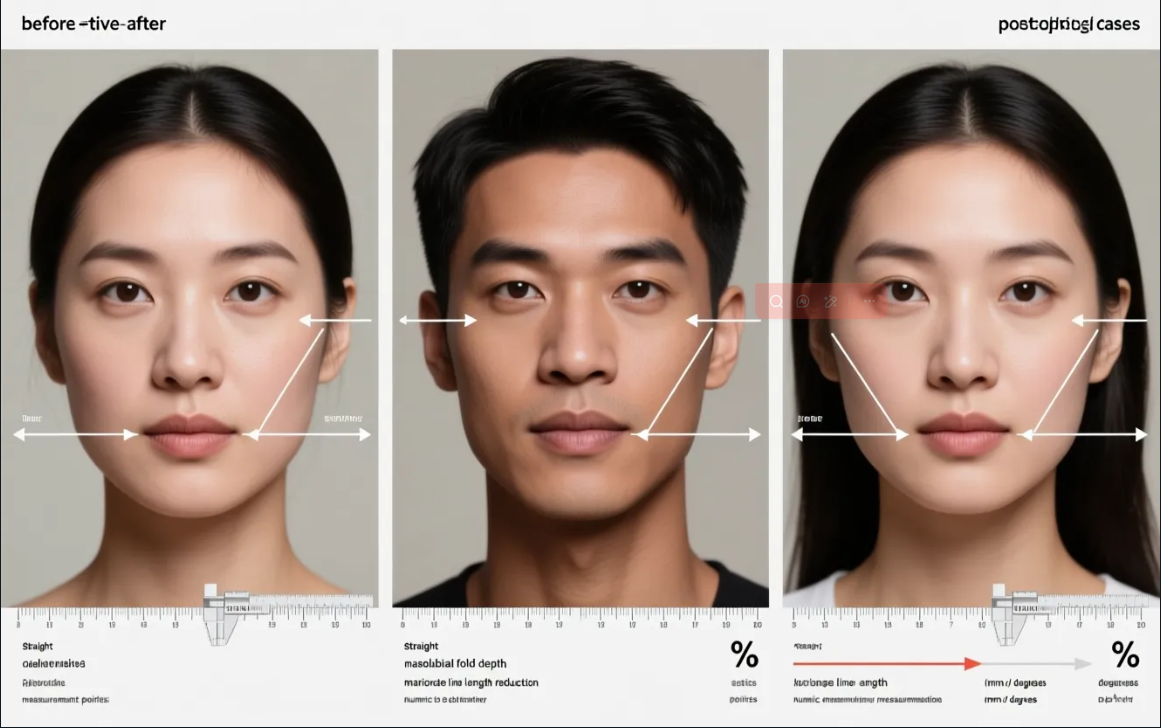
Photographic documentation—standardized two‑dimensional photography and three‑dimensional surface imaging—provides objective morphometric data on changes in jawline definition, midface projection, and nasolabial fold depth. Quantitative measurements can include cheek projection indices, lower‑face vertical dimensions, and angles of mandibular contour. These objective markers, combined with FACE‑Q scores and blinded panel ratings, produce a more robust assessment than surgeon opinion alone.
Case studies and cohort series that pair pre‑ and post‑operative 3D imaging commonly demonstrate that deep‑plane techniques produce measurable midface elevation and increased malar projection compared with more superficial SMAS tightening, particularly in patients with prominent midfacial descent. Such findings support the anatomical rationale for deeper release in appropriately selected patients. However, variability in imaging protocols and follow‑up intervals complicates direct comparisons across institutions.
4. Evidence‑Based Patient Selection Criteria
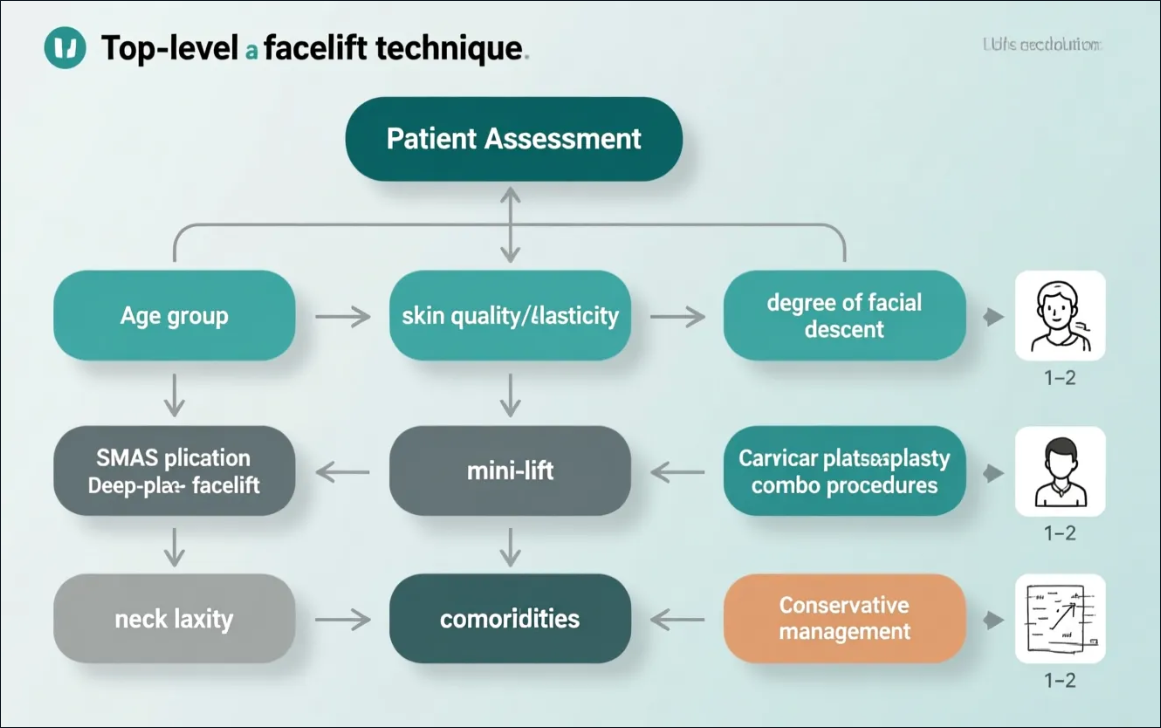
Appropriate technique selection begins with a systematic assessment of patient‑specific factors. Key variables include skin quality, pattern and degree of soft‑tissue descent, vector of desired lift (vertical vs. lateral), patient age and comorbidities, smoking status, and expectations. Integrating these factors into a structured decision pathway improves outcomes and minimizes complications.
Clinical recommendations based on contemporary consensus and expert series include:
- Patients with predominant midface descent, deep nasolabial folds, and significant malar ptosis are often better candidates for deeper plane release (deep‑plane or extended SMAS mobilization) to achieve sustained midface elevation.
- Patients with primarily lower‑face and neck laxity, good skin elasticity, and lower operative risk may achieve excellent results with SMAS plication or limited incision approaches, with shorter operative time and faster early recovery.
- Patients with significant medical comorbidities, bleeding risk, or unwillingness to accept longer recovery should be counseled toward less invasive options (mini‑facelift variants, adjunctive skin tightening technologies, or staged procedures).
- Smoking cessation for several weeks pre‑ and post‑operatively, optimization of medical comorbidities (e.g., diabetes control), and medication reconciliation to minimize anticoagulant exposure are essential risk‑reduction strategies.
Contraindications and relative risk factors should be discussed openly. Active smokers, patients with uncontrolled cardiovascular disease, or those on therapeutic anticoagulation require individualized risk mitigation and may benefit from conservative or staged approaches. Shared decision‑making tools and standardized consent forms that include institution‑specific complication data improve informed consent quality.
Conclusion
Both deep‑plane and SMAS plication facelifts remain valuable techniques in the contemporary surgeon’s armamentarium. Deep‑plane approaches provide anatomical advantages for midface rejuvenation and may offer longer durability in appropriately selected patients; SMAS plication and limited‑dissection methods offer efficient, reproducible results with shorter early recovery and favorable safety profiles for many candidates. Objective outcome assessment using validated instruments (e.g., FACE‑Q), consistent photographic and 3D imaging protocols, and transparent complication benchmarking are critical to advancing evidence‑based practice. Future directions include prospective comparative studies, improved standardization of outcome metrics, and continued integration of imaging and patient‑reported outcomes to tailor procedures to individual anatomy and aesthetic goals.
For clinicians seeking practical resources, professional society pages and outcome registries (e.g., ASPS, The Aesthetic Society) and validated outcome tools (FACE‑Q) are recommended starting points: https://www.plasticsurgery.org, https://www.theaestheticsociety.org, https://www.qportfolio.org/face-q/. Ongoing appraisal of the literature and registry data will refine patient selection and enhance long‑term safety and satisfaction.